Heparin is an anticoagulant frequently used for the prevention and treatment of thrombosis and thromboembolism in hospitals and outpatient clinics. Along with complications of heparin therapy such as bleeding, the development of heparin-induced thrombocytopenia syndrome (HIT) has received considerable attention in recent years. HIT is classified into types 1 and 2.
Type 1 HIT is not immunologically mediated and may be caused by direct platelet activation by heparin. This reaction may develop within the first few days of initiating heparin therapy in approximately 10% of patients. It is characterized by a transient to moderate decrease in platelet count, followed by a rapid recovery within a few days. This reaction is not associated with the development of specific antibodies or thrombosis. Of course, the development of type 2 HIT is of greater clinical significance.
Among patients receiving various types of heparin, this syndrome may develop in 0.5–2% of those receiving unfractionated heparin (UFH) and up to 0.1–0.5% of those receiving low molecular weight heparin (LMWH). Importantly, thrombosis is observed in more than 50% of patients, within 30–50 days of the onset of thrombocytopenia.
Thrombotic complications can manifest as occlusions of arteries in the upper extremities, arteries in the lower extremities, and subsequent gangrene of the hands, feet, fingers, and toes; hemorrhagic necrosis in the thighs and anterior abdominal wall; and cerebral and myocardial infarctions. One of the main laboratory signs of HIT development is a decrease in platelet count to an average of 50%–60% of the initial level, occurring within 5–15 days of initiating heparin use, as well as the detection of specific IgG, IgM, and IgA antibodies in the blood.
Currently, the most widely accepted mechanism for the development of type 2 HIT is the following: Platelet factor 4 (platelet antiheparin factor, TF4), a tetramer, is released from platelet alpha granules in response to the presence of heparin molecules in the blood. The nature of the release reaction depends on the molecular weight, length, and sulfation of the heparin molecule.
When a heparin molecule contacts the TF4 tetramer, conformational changes in the complex occur, creating epitopes to which IgG, IgM, and IgA antibodies are formed. In asymptomatic cases of HIT type 2, IgM and IgA antibody levels are most often elevated. In the classic symptomatic development of HIT type 2, IgG antibody levels are most elevated, although other antibody classes may also be observed. The TF4-heparin-antibody complex then activates platelets through interaction with their FcγIIa receptors, resulting in platelet aggregation, the release of procoagulant microparticles, and the activation of monocytes and leukocytes.
In addition to its reaction with heparin, TF4 can form complexes with heparin-like compounds found in vascular endothelium—heparan sulfates. These complexes, in turn, can be targets for specific antibodies, leading to endothelial damage, activation of the coagulation cascade, thrombin generation, and thrombus formation.
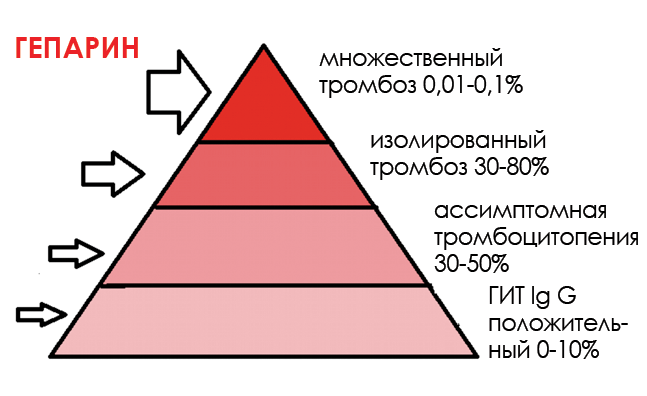
According to the so-called «iceberg» scheme, up to 10% of patients receiving heparin therapy may have specific IgG antibodies in their blood, of which only 30-50% may develop asymptomatic thrombocytopenia. In turn, 30-80% of these patients may develop isolated thrombosis, and multiple thrombosis may be observed in 0.01-0.1% of patients in this group.
Of course, it should be noted that in groups of patients receiving LMWH therapy, the incidence of type 2 HIT was noted to be 10–15 times lower than in patients receiving UFH.
Diagnostics
Diagnosing the development of HIT is quite complex and should primarily be considered a clinical and laboratory process. This complexity is primarily determined by the potential for overdiagnosis of HIT. Thrombocytopenia may be a consequence of iatrogenic influences, especially in intensive care unit patients, or the nonspecific effects of certain medications.
In accordance with this approach, the so-called «4 T scoring system» is used, which is a table of clinical features and their corresponding scores. These features are: thrombocytopenia, time of thrombocytopenia onset, thrombosis, and the presence of alternative causes.
Laboratory diagnostics includes two groups of studies:
· Evaluation of platelet activation and detection of the presence of various classes of specific antibodies in the blood.
Platelet activation is most often assessed by testing platelet aggregation induced by a mixture of heated patient plasma and varying concentrations of heparin. The platelets tested can be either a pool of platelet-rich plasma (PAT test) or a suspension of washed platelets (HIPA test). While these tests are quite specific, they are not very sensitive.
The second platelet activation assessment test (SRA test) is based on the quantitative determination of the release of radioactively labeled serotonin from platelets pre-saturated with serotonin and activated with a mixture of patient plasma and heparin. This test is considered the «gold standard.» Clearly, this research method is quite complex and requires the use of radioactive tracers and appropriate equipment.
The presence of specific antibodies can be detected using several methods:
1.ELISA tests.
2. Direct HIT antibody tests based on antigen detection methods use TF4 complexes (recombinant or platelet-derived) with heparin or polyvinyl sulfonate, followed by evaluation of the antigen-antibody reaction on a solid phase. These methods are offered by Stago, GTI, and HyPHEN BioMed.
3.Immuno agglutination.
4. Membrane immunoassay (PIFA) for rapid diagnostics.
This group of methods evaluates the agglutination reactions of polystyrene particles loaded with heparin-TF4 complexes. Antibodies in a plasma sample are determined by their reaction with these particles as they pass through a gel (PAGIA) from DIAMED or through a membrane (PIFA) from Akers Biosciences.
The relevance of antibody detection is determined by determining a mixture of antibody conjugates or IgG. Several studies have shown that detection of the IgG class of antibodies is the most specific for diagnosing HIT associated with thrombosis. A comparison of this type of assessment with functional methods revealed a closer correlation than with methods detecting a mixture of antibodies.
Along with these data, there are a number of observations of symptomatic HIT occurring in the presence of only IgM or IgA antibodies, particularly in cancer patients. This suggests that the antibody classes with the highest affinity and concentration may be considered pathological.
Thus, the most optimal diagnosis of HIT should be based on the following:
1. Assessment of the number of points on the “4 T scale” (maximum up to 8).
2. Assessment of the kinetics of changes in the number of platelets, more than 30% or less than 100 thousand/ml.
3. A positive platelet activation test, preferably using washed platelets. 4. Determination of the presence of specific antibodies, primarily IgG, using the most sensitive and specific tests. Further comparative studies will help establish and evaluate optimal approaches for increasing accuracy and minimizing the need for laboratory testing in the diagnosis of HIT.
Kosyrev A.B., OOO TPO Medio Lab / Medical Alphabet. Laboratory 1/2011. P. 38.